When Srikanth Singamaneni and Guy Genin, both professors of mechanical engineering & materials science in the McKelvey School of Engineering at Washington University in St. Louis, established a new collaboration with researchers from the School of Medicine in late 2019, they didn’t know the landscape of infectious disease research was about to shift dramatically. In a conference room overlooking Forest Park on a beautiful fall day, the team had one goal in mind: tackle the biggest infectious disease problem facing the world right then.
“Srikanth and I had a vision of a simple, quantitative diagnostic tool, so we connected with infectious disease physicians here at WashU and asked them, ‘What are the most important questions that could be answered if you could get really detailed information cheaply at the point of care?’” said Genin, the Harold and Kathleen Faught Professor of Mechanical Engineering. “Greg Storch told us that one of the most important challenges facing the field of infectious disease is finding a way to figure out quickly if a patient has a bacterial infection and should get antibiotics or has a viral infection for which antibiotics will not be effective.”
Storch, MD, the Ruth L. Siteman Professor of Pediatrics at the School of Medicine, was interested in diseases that affect most people regularly – colds, strep throat or the flu – but that weren’t getting as much research attention as rarer diseases. “Even with great advances that have been made in infectious disease diagnostics, there is still a niche for tests that are simple, rapid and sensitive,” Storch said. “It would be especially powerful if they could provide quantitative information. Tests with these characteristics could be employed in sophisticated laboratories or in the field.”
Research team members Ige George, MD, and Sumanth Gandra, MD, associate professors in the Division of Infectious Diseases at the School of Medicine, noted that the challenge is even greater in resource-limited settings.
“In some of the clinics we work with in India, fast, simple and accurate diagnostic tests at the point of care continue to elude us,” George said. “For example, tuberculosis is one of the leading causes of death in poor countries, where up to one-third of patients are left undiagnosed. For other bacterial infections the costs associated with identifying bacteria and checking susceptibility to antibiotics exceeds the costs of prescribing antibiotics, leading to overuse of antibiotics.”
The problem is not confined to poor countries but also occurs here in St. Louis, added Gandra. “Take gonococcal infection, which has developed resistance to antibiotics over the years. At present, gonococcal infection cannot be diagnosed with simple and highly accurate point-of-care tests. This leads to treatment delays and infection spread,” Gandra said.
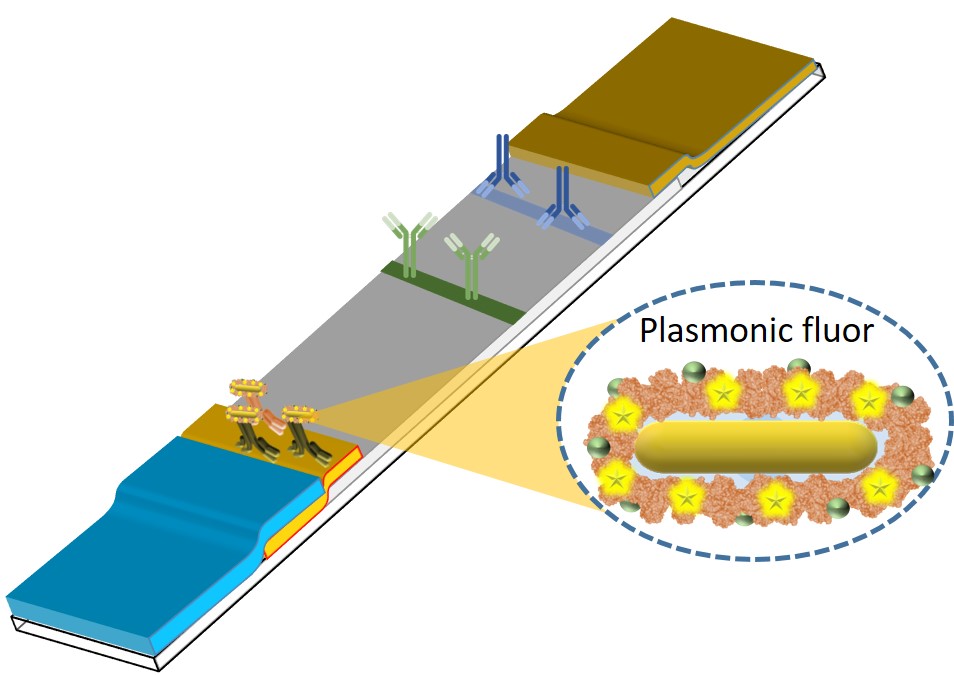
Drawing on his years of experience in developing nanomaterials for applications in biology and medicine, Singamaneni, the Lilyan & E. Lisle Hughes Professor, sought to overcome these limitations in point-of-care diagnostic tests. Singamaneni and his lab developed ultrabright fluorescent nanolabels called plasmonic-fluors, which could be quickly integrated into a common testing platform, the lateral flow assay (LFA). Plasmon-enhanced LFAs (p-LFAs) improve inexpensive, readily available rapid tests to levels of sensitivity required by physicians for confidence in test results without the need for lab-based confirmation.
“The high sensitivity and specificity of the novel biodiagnostic technology combined with its simplicity and low cost make it highly attractive for adoption in the clinical lab and point-of-care settings,” said team member Bijal Parikh, MD, PhD, assistant professor in the Department of Pathology & Immunology at Washington University School of Medicine. Parikh is also the medical director of the Molecular Diagnostics Laboratory.
According to findings published Feb. 2 in Nature Biomedical Engineering, the team’s p-LFAs are 1,000 times more sensitive than conventional LFAs, which show results via a visual color and fluorescence signal on the strip. When analyzed using a fluorescence scanner, p-LFAs are also substantially faster than gold-standard lab tests, returning results in only 20 minutes instead of several hours, with comparable or improved sensitivity. The p-LFAs can detect and quantify concentrations of proteins, enabling them to detect bacterial and viral infections as well as markers of inflammation that point to other diseases.
“Plasmonic-fluors are composed of metal nanoparticles that serve as antennae to pull in the light and enhance the fluorescence emission of molecular fluorophores, thus making it an ultrabright nanoparticle,” Singamaneni explained. “Our p-LFAs can pick up even very small concentrations of antibodies and antigens, typical markers of infection, and give clinicians clear, quick results without the need for specialized equipment. For quantitative testing beyond the initial screening, the same LFA strip can be scanned with a fluorescence reader, enabling rapid and ultrasensitive colorimetric and fluorometric detection of disease markers with only one test.”
“It's like turning up the volume on standard color-changing test strips. Instead of getting a faint line indicating only a positive or negative result, the new p-LFAs give clearer results with fewer particles, enabling one to move from simply ‘yes or no?’ to exactly ‘how much?’ with the aid of an inexpensive, portable scanner,” said Jeremiah Morrissey, research professor in anesthesiology in the Division of Clinical and Translational Research at the School of Medicine. Morrissey is a co-author of the new study and long-term collaborator with the Singamaneni lab.
Co-author Pratik Sinha, MD, PhD, an intensive care and emergency medicine physician also in the Department of Anesthesiology in the Division of Clinical and Translational Research pointed to potential benefits of the new technology. “The LFA technology and inexpensive reader can be readily adapted to the intensive care unit or the emergency room where rapid determination of a patient’s medical condition can be used to tailor appropriate treatment and determine the efficacy of treatment,” Sinha said. “Given how relatively inexpensive it is compared to standard assays, the potential for this technology can be global.”
This improved testing capability has obvious benefits for a population now all too familiar with the need for quick and reliable test results and the risk of false negatives.
“When we took on this problem in 2019, we thought our biggest challenge would be getting an adequate number of samples from sick people,” Genin recalled. “Where on Earth could we find a massive set of samples from patients whose symptoms were carefully documented and whose diagnosis was verified by slow and expensive PCR tests?” In a matter of months, COVID-19 would erase that obstacle while introducing a whole host of new challenges and opportunities.
“The pandemic was a big shift for us, like it was for everyone,” said first author Rohit Gupta, who worked on the p-LFA study as a graduate student in Singamaneni’s lab and is now a senior scientist at Pfizer. “We had to move away from our original focus on distinguishing viruses from bacteria, but it turned out to be an opportunity to do practical science with real stakes. We were working with epidemiologists to get samples for testing, with diagnosticians to compare our test to what was available, and with clinicians to gain insights into the real needs for patient care.”
Input from the entire collaboration helped Gupta and Singamaneni refine the design of the p-LFAs, which ultimately achieved 95% clinical sensitivity and 100% specificity for SARS-CoV-2 antibodies and antigens. Genin described the results as stunning.
“We didn’t know it was going to work so well,” he said. “We knew it would be good, but we didn’t know this $1 test with a $300 readout device would be so much better – 10 times better – than state of the art that we all used during the COVID pandemic.”
Now that they’ve proven p-LFAs can outperform standard lab tests in sensitivity, speed, convenience and cost for one disease, the team is looking to develop new applications for the technology, including returning to their original goal of identifying bacterial versus viral infections and getting their diagnostic tool into the hands of physicians around the world.
The p-LFA technology has been licensed to Auragent Bioscience LLC by Washington University’s Office of Technology Management. Singamaneni and Morrissey are among the co-founders of Auragent, a WashU startup.
“We expect to have p-LFAs commercially available in the next one to two years,” Singamaneni said. “Right now, we’re working on improving our portable scanner technology, which adds a more sensitive, fluorescent reading capability to the test strips in addition to the color change that can be seen with the naked eye. We think we can get that cost down to a point where it’s accessible to rural clinics in the U.S. and abroad, which was one of our original goals.”
“We’re also excited about the potential to detect many more diseases than COVID, possibly using a skin patch that can take a painless sample,” Singamaneni added. “This technology has the potential to detect any number of diseases, ranging from STIs to respiratory infections and more, as well as cytokines indicative of inflammation seen in conditions such as rheumatoid arthritis and sepsis.”
Shawn Ballard
engineering.wustl.edu


